Jun 17, 2026
Written by:

Charlotte Coates, MSN, RN, PMHNP-BC
Founding Clinical Lead, Legion Health

TLDR:
SSRIs block serotonin reuptake in the synapse, but therapeutic effects take 2-4 weeks because your brain needs time to adjust receptor sensitivity, not because the drug builds up slowly.
Six SSRIs account for most U.S. prescriptions, each with different half-lives and side effect profiles that clinicians weigh against your medication list and health history.
Common early side effects like nausea and headaches often fade within weeks, but sexual side effects can persist longer.
Stopping an SSRI abruptly can trigger discontinuation syndrome with symptoms like dizziness and brain zaps; gradual tapering with your prescriber reduces this risk.
Legion Health clinicians conduct full assessments before prescribing SSRIs for Texas adults, accounting for co-occurring conditions like ADHD or anxiety.
Your doctor writes an SSRI prescription, you pick it up, and then you wait. Two weeks pass. Maybe three. You feel nothing different, or something slightly off, and you start wondering whether the drug is even doing anything. This guide explains what SSRIs do in the hours after your first dose, why the therapeutic effects take so much longer to appear, and what to expect if you need to stop.
SSRIs are described as drugs that increase serotonin, but that explanation skips over the most important part. What are SSRIs actually changing in your brain when you take them every day for a month before anything feels different? How do SSRIs work if serotonin levels rise within hours, but depression or anxiety symptoms don't budge for weeks? The SSRI mechanism involves a two-stage process: the drug blocks reuptake right away, and your brain slowly recalibrates its receptor networks in response. Understanding how that receptor adaptation works helps explain why the timeline feels so long and why stopping abruptly can trigger withdrawal symptoms even though SSRIs aren't addictive.
What SSRIs Are and What They Treat
Selective serotonin reuptake inhibitors, or SSRIs, are a class of antidepressant medications that affect serotonin signaling in the brain. They're the most widely prescribed antidepressants in the United States, largely because they tend to be better tolerated than older drug classes like tricyclics or MAOIs.
The "antidepressant" label undersells how broad their clinical use actually is. SSRIs carry FDA approval for conditions including:
Major depressive disorder (MDD)
Generalized anxiety disorder (GAD)
Social anxiety disorder
Panic disorder
Obsessive-compulsive disorder (OCD)
Post-traumatic stress disorder (PTSD)
Premenstrual dysphoric disorder (PMDD)
Not every SSRI covers every condition on this list. Which drug a clinician chooses depends on the specific approval profile, the patient's history, and other clinical factors unique to that person.
How SSRIs Work: The Reuptake Inhibition Mechanism
When a neuron releases serotonin into the synaptic cleft, a portion of that serotonin gets pulled back into the sending neuron through a transport protein. SSRIs block that transporter, so serotonin lingers longer in the synapse and has more opportunity to bind to receptors on the receiving neuron.
The word "selective" matters here. SSRIs target the serotonin transporter and leave dopamine and norepinephrine transporters largely alone. That selectivity is what separates them from older tricyclic antidepressants, which blocked multiple transporters and receptors at once and carried a heavier side effect burden.
One thing worth knowing: the reuptake blockade occurs within hours of the first dose, but most people do not notice mood changes for 2 to 4 weeks. Researchers believe this lag reflects downstream receptor changes that take time to settle, not a slow buildup of the drug itself.
What "increased serotonin availability" actually means
Higher synaptic serotonin availability does not mean the brain simply has more of it. What changes is how long serotonin stays active in the gap between neurons before being cleared. The picture is more complicated than the common shorthand suggests.
The serotonin transporter (SERT) is the direct target. SSRIs bind to SERT and reduce the rate of serotonin clearance, extending the time during which it can activate postsynaptic receptors. At therapeutic doses, SSRIs typically occupy 70 to 80% of available SERT sites, which is why serotonin stays in the synapse longer instead of being cleared immediately after release.
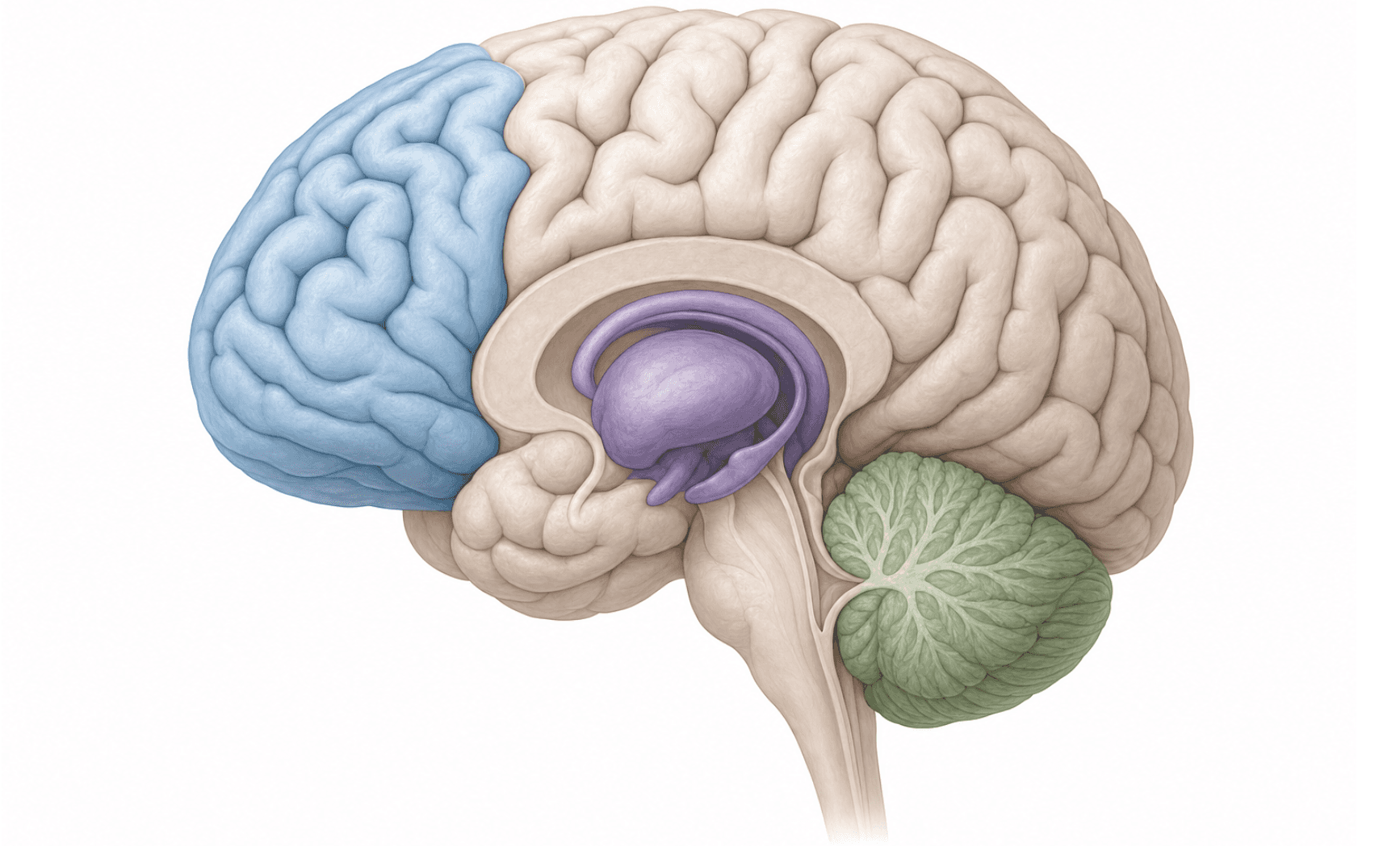
This extended presence does not translate to a flat increase in serotonin signaling. The brain reads high synaptic serotonin as a signal to pull back: postsynaptic serotonin receptors may downregulate in density or sensitivity over weeks of exposure. One leading hypothesis holds that this receptor adaptation, and not the initial blockade itself, is what produces therapeutic effects, given that this recalibration appears to track most closely with when mood changes tend to appear, though the precise mechanism remains an active area of research.
A second feedback loop is thought to run through the raphe nuclei, the brainstem regions where most serotonin-producing neurons are clustered. Presynaptic autoreceptors are believed to detect rising serotonin levels and initially reduce the amount of new serotonin released, partly offsetting the reuptake block in the early weeks, though the degree and consistency of this effect continues to be studied. As those autoreceptors gradually desensitize with continued treatment, serotonin transmission across the relevant circuits may increase more consistently.
The net result is that "more serotonin available" is shorthand for a system that is slowly recalibrating across multiple receptor types and brain regions, not simply running at a higher baseline level from day one.
Why SSRIs Take Weeks to Show Full Effects
One of the most common questions people have after starting an SSRI is why they feel nothing for weeks. The answer comes down to how the brain actually adapts to the change in serotonin availability.
When serotonin levels rise in the synapse, the brain reads this as an overload and responds by pulling back. Serotonin receptors downregulate, meaning the brain reduces the number of receptors that are active or their sensitivity. This is a compensatory response, and it takes roughly two to four weeks to stabilize.
The receptor adaptation timeline
Three overlapping processes unfold during this window:
Serotonin rises almost immediately after the first dose, but presynaptic autoreceptors are believed to detect this increase and reduce further serotonin release, partly offsetting the early gain, though the precise degree of this effect varies across individuals and remains under study.
Over the following weeks, those autoreceptors gradually desensitize, allowing serotonin transmission to increase more consistently across the relevant neural circuits.
Postsynaptic receptor density adjusts in parallel, and this slower recalibration appears to track most closely with when people begin noticing mood changes.
This is why the clinical window for assessing whether an SSRI is working is usually four to six weeks at a therapeutic dose, not the first few days.
Common Types of SSRIs Prescribed in the United States
These six SSRIs account for the vast majority of prescriptions written in the United States. They share the same core reuptake inhibition mechanism, but their half-lives, receptor activities, and drug interaction profiles differ enough that clinicians consider each separately instead of treating them as interchangeable options.
Generic name | Common brand name | Approximate half-life | Notable clinical characteristics |
|---|---|---|---|
Fluoxetine | Prozac | 1 to 6 days (active metabolite) | Longest half-life of the class; lower discontinuation risk |
Sertraline | Zoloft | ~26 hours | Broad FDA approval profile across several conditions |
Paroxetine | Paxil | ~21 hours | Shorter half-life; anticholinergic activity; higher discontinuation risk |
Citalopram | Celexa | ~35 hours | FDA dose ceiling in place due to QT interval concerns |
Escitalopram | Lexapro | ~27 hours | S-enantiomer of citalopram; generally fewer drug interactions |
Fluvoxamine | Luvox | ~15 hours | Primarily approved for OCD; strong CYP enzyme inhibition |
How clinicians choose between them
Selecting an SSRI is rarely straightforward. A clinician will weigh a patient's full medication list, other health conditions, and prior treatment responses before landing on a specific drug. Fluoxetine's long half-life, for example, can make it a practical choice for patients who frequently miss doses, while the same property makes it a poor fit when a fast washout period is clinically important.
Side Effects: What to Expect and How Common They Are
SSRIs are generally well-tolerated, but they do come with side effects that vary by person and medication. Knowing what to expect can help you and your clinician decide whether a given SSRI is a good fit.
The most common side effects tend to appear early in treatment and often improve within a few weeks:
Nausea and gastrointestinal upset, which can show up in the first week or two, usually settle as your body adjusts.
Headaches and fatigue, especially in the first few days after starting or increasing a dose.
Sleep changes, including insomnia or vivid dreams, which some people notice early on.
Sexual side effects, such as reduced libido or difficulty reaching orgasm, are among the most common and may persist longer than other side effects.
Some side effects are less common but worth knowing:
Increased anxiety or restlessness shortly after starting, which can feel counterintuitive but typically fades within the first couple of weeks.
Weight changes over longer treatment periods, though the pattern varies by specific medication and individual.
Your clinician can adjust timing, dose, or switch medications if side effects become unmanageable. No SSRI works the same way for every person, so finding the right fit may take some trial and adjustment.
Serotonin Syndrome: Recognizing a Rare but Serious Risk
Serotonin syndrome occurs when serotonin activity in the brain and body reaches toxic levels, usually after combining two or more serotonergic drugs. It can range from mild discomfort to a life-threatening emergency, and onset is often rapid.
What to watch for
The condition produces three overlapping categories of symptoms:
Neuromuscular changes: muscle twitching, rigidity, or uncontrolled movements that are hard to suppress voluntarily
Autonomic instability: racing heart, high blood pressure, fever, and heavy sweating that appear together and escalate quickly
Altered mental status: agitation, confusion, or restlessness that feels distinct from typical anxiety
Common triggers
Risk rises sharply when SSRIs are combined with other serotonergic agents, including other antidepressants, certain pain medications like tramadol, and some migraine treatments called triptans. Starting a new medication or increasing a dose are the most common precipitating events.
If you experience any of these symptoms after a medication change, seek emergency care right away. A clinician assessing you for SSRI treatment can review your full medication list to identify combinations that may increase risk before you start.
Special Considerations: Drug Interactions and Safety Warnings
SSRIs are generally well tolerated, but a few safety considerations are worth knowing before starting treatment.
The most common early side effects include nausea, headaches, insomnia, and sexual dysfunction. These often ease within the first few weeks as the body adjusts.
One warning that applies to all antidepressants is the FDA black box warning on suicidal thoughts, particularly in people under 25. This risk appears highest in the early weeks of treatment, which is why clinicians typically schedule close follow-up after a new prescription.
Drug interactions to flag with your prescriber
Combining SSRIs with other serotonergic drugs, including tramadol, triptans, or certain supplements like St. John's Wort, can raise the risk of serotonin syndrome, a potentially serious condition involving agitation, rapid heart rate, and high body temperature.
Monoamine oxidase inhibitors (MAOIs) should never be taken alongside SSRIs due to the risk of severe, potentially fatal serotonin toxicity.
Some SSRIs inhibit liver enzymes that process other medications, which can raise or lower the blood levels of drugs taken at the same time.
If you are starting an SSRI, bring a full medication and supplement list to your appointment. A clinician can assess your full picture before prescribing.
Stopping SSRIs: Discontinuation Symptoms and Tapering
Stopping an SSRI abruptly often triggers a cluster of symptoms known as discontinuation syndrome (dizziness, nausea, irritability, and distinctive electrical jolts). This is separate from addiction. The brain has adapted to a new serotonin signaling baseline, and cutting off the drug suddenly creates a rapid shift it has no time to adjust to.
These typically begin within a day or two of a missed or stopped dose. For many people, they fade within a few weeks, though the timeline can vary considerably depending on the person, the medication, and how long they were on it.
Because paroxetine has one of the shortest half-lives in the class, it carries a much higher discontinuation risk compared to fluoxetine, which clears the body far more slowly and often produces milder or no discontinuation symptoms. A clinician can account for these differences when building a tapering plan.
There is no universal tapering schedule. The right pace depends on how long you have been on the medication, your current dose, and how your body responds to tapering. Standard psychiatric prescribing guidance is clear that tapering should be gradual and supervised.
If you are considering stopping an SSRI, work with your prescriber instead of stopping on your own. Dose reduction over several weeks reduces symptom severity, and your clinician can slow the taper further if symptoms become difficult to manage.
How Legion Health Approaches SSRI Prescribing in Texas
Legion Health works with patients starting an SSRI for the first time and those reconsidering a prescription that stopped working. Board-certified psychiatric clinicians conduct full evaluations before prescribing, accounting for co-occurring conditions and any physical health factors that may affect treatment.
When ADHD overlaps with depression or anxiety, a clinician assesses which conditions are present and how they interact before building a treatment plan. ADHD evaluations include QbCheck, an FDA-cleared objective test, at no extra cost alongside the clinical interview.
For Texas adults, new patient appointments are typically available within three to five days. Most patients pay around a typical specialist copay using their Texas insurance plan.
Final Thoughts on SSRI Mechanisms and Treatment
The core mechanism is simple: SSRIs prolong serotonin's time at the synapse. What happens after that is more complicated, and it explains why these medications take weeks to work and why tapering matters when you stop. If you're weighing whether to start or stop an SSRI, working with a psychiatric clinician gives you a clearer picture of what to expect and how to manage the process safely.
FAQ
How do SSRIs work?
SSRIs block the serotonin transporter protein, slowing serotonin reuptake and prolonging the time serotonin remains active at the synapse between neurons. This mechanism happens within hours, but therapeutic effects typically take two to four weeks as postsynaptic receptors downregulate, and the brain adapts to the new signaling environment.
SSRI mechanism: Prozac vs Zoloft vs Lexapro?
All three use the same reuptake inhibition mechanism targeting the serotonin transporter, but Prozac has a much longer half-life (1 to 6 days), making it easier to stop, while Zoloft has broad FDA approval across multiple conditions, and Lexapro typically has fewer drug interactions. Your clinician will choose based on your medication list, health conditions, and treatment history.
Can I stop taking an SSRI without tapering?
No. Stopping abruptly often triggers discontinuation syndrome: dizziness, nausea, irritability, and electrical-jolt sensations. This happens because your brain has adapted to altered serotonin signaling and needs time to readjust. Work with your prescriber to build a gradual tapering schedule over several weeks.
What are SSRIs used for besides depression?
SSRIs carry FDA approval for generalized anxiety disorder, social anxiety disorder, panic disorder, OCD, PTSD, and premenstrual dysphoric disorder, though not every SSRI is approved for every condition. Which medication a clinician prescribes depends on the specific approval profile and your individual clinical picture.
When should I expect an SSRI to start working?
Most people notice mood changes two to four weeks after starting treatment, not within the first few days. The delay reflects postsynaptic receptor adaptation and autoreceptor desensitization, which take time to stabilize even though serotonin levels rise almost immediately after the first dose.
This article is for informational purposes and is not medical advice. If you think you may have symptoms of a mental health condition, a psychiatric evaluation can help.
How legion health Can Help You
If you’re in perimenopause or menopause and want guidance from clinicians who specialize in women’s midlife health, book a virtual visit with Legion Health today.
Hormonal changes are at the root of many symptoms women experience in the years before and after their periods stop.
Our trained menopause specialists help you connect the dots and guide you toward safe, effective solutions.
Whether you need personalized care or a prescription-based treatment plan to manage symptoms—including brain fog, hot flashes, sleep issues, mood swings, and weight gain—we’ve got you covered. Learn more here.
We're honored to support thousands on their journeys. Here's what some have shared: